{kind=link}
Please contact Dr. M Hewson
Download from www.specialcare.app
Future updates will install automatically
This version:
For use only in conjunction with the relevant NALHN and State-wide guidelinesClose
This app is designed to assist with your orientation to the Special Care Nursery and Women's Health wards.
Use this information alongside the relevant Practice Guidelines.
More than 3800 births per year
Cesarean Rate 28%
More than 250 births per year under 37 weeks
Level 5 nursery
16 funded beds - flex up to 24 beds
4 High Dependency beds
GA 31 weeks, Birth Weight 1500 grams
Infants born at LMH below these thresholds will be transferred to WCH for initial care
GA less than 36 weeks, OR Birth Weight less than 2300 grams
Are to be admitted to SCN unless otherwise discussed with the Neonatologists or Paediatrician
(About 15% of newborns 2200 - 2300g will avoid admission)
CGA ≥ 31 weeks
Current weight ≥ 1350 grams
Full enteral feeds
Resp support no greater than High Flow 25%
We run regular NLS and NALS sessions.
Please book into NLS or NALS courses via your iLearn account
NLS & NALS course schedule
Handover in Special Care Nursery at 08:00
Followed by SCN Ward Round
Wednesday Ward Round is led by the Registrar
Reg and RMO share clinical duties in nursery. Infants examined at least twice per week (once each by Reg and RMO) with exam results documented.
Plot growth charts every Monday
Brief consultant afternoon round usually about 15:30 - 16:00
20:30 Handover to Night Registrar. Highlight possible discharges for next day.
Handover from Registrar in SCN
Review unwell infants in nursery
The registrar is expected to take an active role in reviewing infants admitted in the last few days: Common issues to consider include:
Attend cesareans and resuscitations on Birthing Unit
Update EMR handover and any pending discharges
In the morning present new admissions to the Handover Round
Finish at 08:30
Handover in Special Care Nursery at 08:00
Attend to newborn checks / reviews in birthing unit first
Check list of discharge checks and reviews on Women's Health Ward
Do checks for imminent discharges first to help with patient flow
Get help from Resus Reg if busy
Consult with Resus Registrar for any queries
Handover in Special Care Nursery at 08:00
Get the Resus pager from the night registrar
Notify Co-ordinator & Neonatologist on SCN re anticipated admissions
Attend relevant cesareans and newborn resuscitations
Help with postnatal ward and birthing unit discharge checks when possible
Monday 12:30 - 13:30 (alternate weeks)
Dr Sthavan will notify you of your turn to present.
Topics alternate beween Paeds and Neonatal
Discuss with one of the neonatologists if you need help with article selection
Or look at Keith Barrington's Neonatal Research blog if you want inspiration
Wednesday 13:00 - 14:00 in Tutorial Room
On first Wednesday of the month the SCN Day Shift Registrar will be presenting
Week 2: Nursing presentation
Week 3: Safety & Quality presentation
Week 4: Consultant presentation
Friday 13:00 - 14:00 in Tutorial Room
Friday 14:00 - 14:30 (alternate weeks)
The Paediatric Senior Reg will arrange the list of cases
Use the "Discharge Summary, Medical" document template rather than the "Neonatal Discharge Summary" for creating discharge summary for infants discharged from the Special Care Nursery.
Our goal is to complete all discharge summaries on the day of discharge
All Registrars and RMOs on all shifts can assist with updating and completing discharge summaries
Tuesday morning from about 10:00 (with Dr Varghese)
Thursday morning from about 10:00 (with Dr Hewson)
Held in Family Clinic
SCN Day Registrar attends
Or Resus Registrar if no reg in SCN
Discuss any queries with the neonatologist in clinic
Discuss follow up requirements with neonatologist
Or if clinic neonatologist is on leave, the on-service neonatologist is available to provide supervision
Please send copy of clinic letter to parents if possible
A daily clinic for follow-up of investgations such as hip ultrasounds, renal scans or blood results
Where the physical attendance of the infant / family is not required
Infants are booked in using the booking form available in SCN and on Women's Health
You will also need to book or arrange the required ultrasound or blood test
The SCN ward clerk will chase up the timing of the scan and then schedule the Virtual Clinic appointment for the day after the scan (to allow time for reporting).
The SCN ward clerk will print a copy of the Virtual Clinic list every day, and place it in the red tray in the SCN Clinical Handover Room
The SCN Reg/RMO must review the Virtual Clinic appointment list each day (Monday - Friday) and chase up the relevant investigation, and plan further management
Telephone the parent and discuss results and any further follow up
Discuss any concerns or uncertainties with the on-service Neonatologist
Document your plan in the EMR using a Neonatal Clinic Note
The on-call Consultant for Neonates will be called (by switch) for EVERY Cat One Section
Please let the consultant know if delivery occurs before their arrival and attendance is no longer required
Neonatal Consultant is NOT called to Code Blue Newborn
You will need to specifically call the consultant in if required
Don't just take a photo of the screen with your phone - the image quality will be poor
Instead, copy the image from the computer:
Extension |
You dial |
20xxx |
08 828 20xxx |
21xxx |
08 828 21xxx |
29xxx |
08 818 29xxx |
83xxx |
08 813 83xxx |
35xxx |
08 839 35xxx |
Call Medstar on 13 7827 (13-STAR)
Select Option 1
The Nurse Retrieval Coordinator will answer and will take the basic details (like your name, location, patient name, DOB, weight)
The NRC will then connect you to the Retrieval Consultant Neonatologist
The Consultant will want to know the more detailed clinical picture and will then give clinical advice and will plan the Medstar kids retrieval team
GA at birth < 31 weeks OR
Birth weight < 1500g OR
Otherwise requested by neonatologist
First examination at six weeks
Follow up as determined by ophthalmologist
Eye exams are performed by Dr Swati Sinkar
Examinations on alternate Mondays
GA at birth less than 30 weeks OR
Birth weight less than 1250 grams
First head ultrasound Day 7 - 10
Follow up scans as indicated
GA at birth less than 32 weeks OR
Birth weight less than 1500 grams
Note that there are many infants outside these criteria who will also be followed up in NNR clinic.
Generally 8 - 10 weeks post-discharge
Confirm timing with Consultant
GA at birth less than 32 weeks OR
Birth weight less than 1500 grams
HIE Grade 2 or 3
Identified syndromes associated with dev. delay
Physiotherapy at 3, 6, 9, 12, and 18 months CGA
Occupational therapy at 12 months CGA
Speech therapy at 18 months CGA
Physiotherapy regularly check our inpatient lists for relevant patients
And will try to see eligible newborn as an inpatient in SCN
Then will arrange MDT follow up
We can also directly refer to MDT via the MR037 (Internal Referral Form for Outpatients)
As a minimum:
FBC, ALP, Ca, PO4 and capillary gas every 4 weeks
Use the "Critical Bloods" kit (found in the SCN)
Kit includes detailed list of tests required, and blood volume required
And includes the blood sample tubes you'll need
Newborn <37 weeks corrected GA: High Alarm 96%, Low Alarm 89%
Newborn ≥37 weeks corrected GA: High Alarm 98%, Low Alarm 91%
Newborn in room air: limits per gestation as above but set high alarm to 100%
When infant is receiving supplemental oxygen, saturations in the high 90s may be associated with hyperoxia
Hyperoxia is a major cause of ROP in preterm infants
Hyperoxia is injurious to the brain (following asphyxia)
Note that infants in room air are not at risk of hyperoxia so sat. upper alarm limits should be set to 100%
CPAP recruits alveoli, and reduces work of breathing
CPAP reduces the need for up-transfer compared to incubator oxygen
FiO2 over 25%
Any supplemental oxygen requirement in newborn under 36 weeks
Any supplemental oxygen requirement in newborn with more than mild indrawing
If intubation required, give surfactant
If on CPAP with FiO2 > 30% despite at least 6 cm CPAP to maintain sats 90 - 95% then give surfactant
Dose is 200 mg/kg
FiO2 over 30% despite CPAP 6cm
to maintain sats 90 - 95%
give surfactant
Dose is 200 mg/kg
Drug room bench on charging dock
Blades (size 0 & 1) in bottom right corner cupboard
Simple on/off button
Blades are single use only
Touch screen icons to record video or still image
See attached document for information on recording intubations for review
And guidance on optimal use for best results
Ventilation (beyond just a few minutes) is infrequently required at LMH SCN.
Typical scenarios include extreme preterm infant with RDS, severe meconium aspiration, significant encephalopathy, or severe sepsis.
We keep one of the Drager VN-500 ventilators in "stand-by" ready to use
Ensure the humidifier has been turned on and has water added before ventilating
Heating and humidifying the ventilator gases is essential for health of ventilated lungs
The VN-500 is set on PC-AC mode
PC means the ventilator delivers set pressures
AC means the ventilator allows the infant to trigger additional ventilator breaths
PIP (peak inspiratory pressure) is set at 20 cm H2O
PEEP is set at 5 cm H2O
Rate is 50/min
Ti (inspiratory time) is set at 0.33 seconds
The VN-500 measures the VT - the volume of each breath
This is a very useful real-time insight into adequacy of ventilation
Generally we want VT of 5 mL /kg
Adjust PIP as required to keep VT near this value
PIP should be increased or decreased to achieve appropriate VT (based on infant weight)
It's not unusual to need PIP of up to 30 cm in conditions of low lung compliance. Pressures above 35 cm are seldom required.
Remember that the set rate is only a back up rate - if the infant is triggering more breaths then altering the back up rate may have little effect
If saturations are poor despite high FiO2 and sensible VT, consider longer Ti (eg 0.4 seconds) or increased PEEP (to 5.5 or 6)
VT provides real-time insight into ventilation
Capillary (or venous) gases give information about adequacy of ventilation though measured CO2 will somewhat exceed true arterial CO2
Low CO2 may be appropriate compensation in cases with significant metabolic acidosis
Pre-ductal oxygen saturations should be maintained in mid-90s to prevent hypoxia and hyperoxia (noting that hyperoxia is a real risk for both very preterm infants and infants at risk of encephalopathy)
Doctor / NP obtain written consent from parent
Doctor / NP writes prescription in the morning
Pharmacy ring when ready
Midwife collects from pharmacy
Pending administration vaccine stored in vaccine fridge in labour ward (because no suitable fridge in SCN)
Immunisations generally administered around 5 AM - 6 AM
Preterm infants have an increased risk of cardio-respiratory instability after immunisation
Cardio-respiratory monitoring should be performed for the first 48 hours post immunisation
Engerix B Paediatric OR H-B-Vax II Paediatric |
IM |
0.5 mL |
Within 7 days of birth (ideally within 24 hours) |
||
No catch-up required |
||
Infanrix Hexa |
IM |
0.5 mL |
hepB-DTPa-HiB-IPV |
||
Prevenar 13 |
IM |
0.5 mL |
Pneumococcal conjugate (13vPCV) |
||
Rotarix |
oral |
1.5 mL |
Rotavirus |
||
Bexsero |
IM (Left leg) |
0.5 mL |
Meningococcal B |
||
Prescribe paracetamol also: first dose 30 minutes prior to immunisation, followed by two more doses (see paracetamol guideline for dose and interval details). Note that dosing interval of 6 hours is not appropriate for younger gestations |
||
Bexsero is to be administered to LEFT anterolateral thigh |
||
All doses must be prescribed as caffeine citrate
1 mg caffeine = 2 mg caffeine citrate
Standard |
20 mg/kg |
Maximum |
80 mg/kg |
5 - 10 mg/kg/dose every 24 hours, commencing 24 hours after the loading dose |
|
Maintenance doses of up to 20 mg/kg have been used |
Discontinue at 34 weeks (unless significant apnoea continues) |
|
Monitor infant for 5 days after ceasing caffeine |
Gestation at birth < 32 weeks |
|
OR birth weight < 1500 grams |
Continue until 34 weeks of corrected age
≤ 1.5 kg |
3 mg/day elemental iron (0.5 mL/day Ferro-liquid) |
1.5 - 3 kg |
6 mg/day elemental iron (1 mL/day Ferro-liquid) |
> 3 kg |
9 mg/day elemental iron (1.5 mL/day Ferro-liquid) |
Ferro-liquid contains 30mg elemental iron per 5ml |
|
Chart as ml of Ferro-Liquid |
|
2 - 6 mg/kg/day elemental iron (0.3 - 1 ml/kg/day Ferro-liquid) |
|
If on preterm formula / fortified EBM consider 3 mg/kg/day elemental iron (0.5 ml/kg/day Ferro-liquid) |
Prophylactic iron indicated if birth weight < 2000 grams OR GA at birth < 34 weeks |
|
Commence at 4 weeks once tolerating full enteral feeds |
|
Not needed if on fortified EBM or preterm formula UNLESS iron deficiency / significant anemia |
|
Breast fed: Continue to 6 months CGA |
|
Formula fed: Continue to 3 months CGA |
Analgesic / antipyretic
250 mg in 5 mL oral liquid
20 mg/kg
Followed by maintenance at next dosing interval
28 - 32 weeks CGA |
15 mg/kg |
12-hourly |
33 - 36 weeks CGA |
15 mg/kg |
8-hourly |
≥37 weeks CGA |
15 mg/kg |
6-hourly |
Birth weight < 2000 grams OR GA at birth < 34 weeks |
|
Mother with known Vitamin D deficiency |
|
Mother at risk: dark skin, veiled, house bound, recent refugee arrival |
6 months (or continue for 12 months if maternal risk factors)
If maternal vitamin D deficiency (< 30 mmol/L) was noted in third trimester (and hence untreated or partially treated) consider Ostelin 0.4 mL daily for the first 3 months, followed by 0.2 mL daily until 12 months
Note that this feed thickener is predominantly maltodextrin which is a fully digestible carbohydrate with 4 kcal per gram
Thus our typical dosage increases caloric value of milk by about 10%
If prescribing enteral feeds on Day 1, generally 40 mL/kg/day is sufficient to meet minimal water and energy requirements.
This reduces the risk of feed intolerance and vomiting that might occur with higher rates.
Day 1 generally 60 mL/kg/day using Glucose 10% without additives
Restrict to 40 mL/kg/day in HIE
For infants with documented hypoglycemia AND at risk of hyperinsulinism, start iv fluids at 90 mL/kg/day Glucose 10% and titrate up or down with blood sugars.
Consider central access (UVC) and use of more concentrated glucose solutions. Discuss with consultant.
Usually advance by 20 - 30 mL/kg/day
Serial weight, clinical examination, and serum Na+ results will guide decision-making.
From 48 hours change iv fluids to premix Glucose 10% with KCl 10 mmol/500 mL and NaCl 0.225%.
Note this solution contains 19 mmol NaCl per 500 mL
Use the original version of Neonatal Early Onset Sepsis Calculator for infants 34 weeks and above and no more than 12 hours of age.
If using calculator select baseline EOS Incidence of 0.8 per 1000 live births as this reflects the most current Australian data
We don't have data on the EOS rate specifically for infants 34 weeks and up: the figure will be somewhat lower than the all-live-births figure quoted above, since EOS (particularly due to gram negative organisms) is much more common in extreme prematurity.
Take a minimum of 0.5 mL. Any lower volumes risk a false negative blood culture
Blood cultures in EOS will report positive in 80 to 100% of cases within 24 hours of the culture bottle going into the incubator
If the culture is negative 24 to 36 hours after reaching the incubator and the clinical scenario is not otherwise concerning for sepsis we generally cease antibiotics.
When red cells are required acutely to treat acute severe hypovolaemia due to blood loss:
Blood bank will then deliver the requested product urgently to the stated location without the prior need for a transfusion request form
Blood Product |
Required |
Recommended |
Uncrossmatched O Neg |
Emergency |
|
Leucocyte depleted |
All red cell transfusions |
|
Irradiated |
History of in utero transfusion |
Birth weight < 900g or GA at birth < 28 weeks |
CMV Negative |
Immuno - compromised |
Any Preterm |
Guidelines for non-acute transfusion in ex-prems:
The table gives the applicable Hb threshold below which transfusion is generally recommended
Usual volume: 15 - 20 mL/kg over three to four hours. Frusemide is seldom required.
Sample |
CPAP > 30% O2 |
Lesser resp support |
Capillary |
100 |
85 |
Art. or venous |
90 |
75 |
| For pre-discharge infants, reduce these thresholds by 5 g if retics ≥ 5%. Reduce by a further 5 g if infant is completely asymptomatic |
||
To document a well newborn discharge check on the EMR, follow these steps:
Note: Do NOT use the "Neonatal Discharge Summary" document type to document the discharge examination of the well newborn.
The well newborn never admitted to the nursery does not require a medical discharge summary.
A quick run through of the standard elements of newborn discharge exam
View on desktop computer: the website uses flash and won't run on most mobile phone browsers
Watch from 13 - 24 minutes for key how-to. The entire video is worth watching.
Abnormal findings are:
Note that while the fundal reflex is typically red in infants with fair skin colour, the fundal reflex colour is typically paler with yellow or white colours in black infants
Discuss any concerns with newborn eye exam with the Neonatal Paediatrician. Conditions such as congenital cataract are emergencies.
Refer urgently to paediatric ophthalmologist if abnormal fundal reflex
Refer to Paeds opthalmology at WCH
Alternatively Dr Sinkar may be able to see urgently in private clinic (gap charge may apply)
A-P renal pelvis dilation (APRPD) of 7 mm or more
Persistent calyceal dilatation
Dilated ureter
Dilated / thickened bladder
Other concerning features such as cystic dysplastic kidney, reduced amniotic volume (without known cause), malpositioned or duplex kidney, or solitary kidney
APRPD > 15 mm
Bilateral APRPD > 10 mm (the concern is that the infant may have obstructed bladder outlet / posterior urethral valves)
Solitary kidney
Suspected obstructed duplex kidney
Dilated / thickened bladder
Suspected bladder outlet obstruction
Ectopic (pelvic kidney): order ultrasound for Day 3 to 7, and refer to Paeds Urology at WCH (will be seen at 3 months)
Solitary kidney: order ultrasound for Day 3 to 7, and refer to Paeds Nephrology at WCH (will be seen at 3 months)
Antenatal APRPD 7 - 14 mm
With or without central calyceal dilatation
But no other antenatal renal abnormality
Normal exam: routine care
Uncertain / equivocal exam: discuss with neonatologist
Abnormal exam: see below
We no longer request screening ultasound based on risk factors
Clicks are not significant. If unsure either:
Re-examine in a day or two, or
Ask registrar or consultant to examine
Discuss with neonatologist who may order an ultrasound
Refer to Mr Allcock by internal referral form for clinical review at two weeks
(Mr Paul Allcock is the local (LMH) paediatric orthopaedic surgeon)
If still unstable at 2 weeks will treat with Pavlik Harness
If stable at 2 weeks Mr Allcock will arrange 6 week scan
Refer to Mr Allcock via on call ortho registrar
Pavlik harness to be applied before discharge
Book Ultrasound for confirmation
Refer to Mr Allcock via internal referral form
Mr Allcock will attempt closed reduction under GA when old enough
May need open reduction at about 1 year
Graf |
alpha |
beta |
Implications |
1 |
> 60 |
< 55 |
Normal |
2a |
50 - 59 |
< 55 |
Immature: repeat at 3 months |
2b |
50 - 59 |
< 55 |
Persisting at 3 months: urgent referral to Mr Allcock via call to LMH Ortho Reg and internal referral form for Pavlik harness |
2c or worse |
<50 |
≥ 55 |
Urgent referral to Mr Allcock via via call to LMH Ortho Reg and internal referral form for Pavlik harness |
A history of meconium stained liquor is not a contra-indication to early discharge in an otherwise well infant
30 to 50% of murmurs heard are due to CHD
Note that half of newborns with significant CHD don't have a murmur
Perform thorough cardiac exam
Pre- and post-ductal sats
Post-ductal sats should be ≥ 95% in air
4-limb blood pressures only required if femorals abnormal or baby unwell
Ask reg or consultant to examine
Re-examine prior to discharge
Referral to WCH cardiology for echo: if significant concern for congenital heart disease
Follow up in 2 weeks by GP: if examination features are benign
Note that 3 to 4 weeks is typical timing for development of heart failure in moderate to large VSD
Cord lactate > 4 is common (data on 17,000 vigorous newborns)
Cord lactate of 8 equates to pH 7.15 See Gjerris 2008
There's no evidence that a saline bolus improves outcome in normovolemic infant with elevated lactate
Cord lactate 8 or more:
Review at 2 - 3 hours including behaviour (?HIE)
Evaluate sepsis risk (calculator)
Check capillary lactate at 4 hours
No routine repeat lactate if cord lactate < 8
Review at 2 - 3 hours including behaviour (??HIE)
Evaluate sepsis risk (calculator)
Check capillary lactate at 4 hours
No routine repeat lactate if cord lactate <8
Manage as appropriate:
Consider HIE. On-going evaluation.
Evaluate sepsis risk (calculator)
Consider other causes eg anemia
Repeat lactate as clinically indicated
Refer to the form "Subgaleal haemorrhage surveillance observations" (MR 130)
This outlines criteria for observations for infants with or at risk of subgaleal bleed
MR 130 form is available in Special Care Nursery
Always notify neonatal paediatrician urgently if you identify a subgaleal bleed
There is a very good review in J Paed Child Health 2014
See SA PPG (above) for discussion of maternal testing, intrapartum care, and postnatal care
HBIG and HB Vaccine given to baby within 12 hours of birth
Provide infant's parents with a request form for blood testing for HBsAg and HBsAb and Hepattis B core antibody at 12 months of age
Book follow up clinic with Dr Yumin Chan (Paeds ID) to review results at 13 months of age
See guideline for discussion of maternal testing, intrapartum care, and postnatal care including issues around breastfeeding
Overall the risk of transmission to infant is no more than 5%
Perinatal HCV exposure: Give infant's mother a form for Hep C antibodies at 12 months of age and arrange outpatient clinic with Dr Yumin Chan (Paeds ID Clinic) at 13 months
Always discuss these infants with Consultant:
This may represent primary infection which is very high risk to newborn
The mother may still be shedding virus at delivery even if no visible lesions
Protective factors in these cases include
Consider early pre-emptive treatment with aciclovir
Mother with past history of HSV and recurrent genital lesions at delivery:
Surveillance swabs and urine at 24 hours
Appropriate advice to parents re signs of illness
Mother with past history of HSV but no recurrent genital lesions at delivery:
No additional investigations are required
Thrombocytopenia is relatively common in pregnancy
Causes include:
Gestational thrombocytopenia
ITP
PET & HELLP
Commonest cause of maternal low platelets
Maternal platelet count seldom < 100
Entirely benign condition
No risk of neonatal thrombocytopenia
Causes 10% of thrombocytopenia in pregnancy
Maternal platelet count may be below 100
10% of newborns will have platelet count below 50
Newborn platelet nadir may be Day 2 to 5
No need for newborn FBC in gestational thrombocytopenia with maternal platelets > 100
Maternal ITP: obtain neonatal FBC (eg cord)
If newborn platelet count < 150: repeat in 24 hours
Moderate or severe neonatal thrombocytopenia will require appropriate investigation and management
Transplacental passage of thyroid stimulating antibodies (TSHR-Ab aka TRAB) can cause neonatal hyperthyroidism
Between 2% and 12% of infants of mother with Graves develop hyperthyroidism
The newborn usually presents within the first 10 days
A negative maternal screen for TSHR-Ab makes this complication very unlikely
The precise level of TSHR-Ab as measured in 3rd trimester may be very helpful in quantifying the risk in a given newborn.
TSHR-Abs can persist after maternal treatment
If maternal TSHR-Ab negative the risk to infant is low
No TFTs unless symptomatic
No need for extended observation
SCN admission if maternal TSHR-Abs more than 5-fold above top of reference range
Minimum 48 hours observation (on post-natal) before discharge for at-risk
Check TFTs at Day 3 and Day 10
Findings may include:
Tachycardia and heart failure
Low birth weight and poor weight gain
Feeding difficulty
Irritability
Some sources recommend obtaining cord blood for TSHR-Ab levels if maternal testing was not done...
if negative this moves infant to a low risk class (see above).
In practice Cord TSHR-Ab is seldom helpful because the test is only run on Thursdays
Can cause both hyper and hypothyroidism in the newborn
However risk of either is quite low
No more than routine Guthrie screening required
If due to treatment of previous Graves Disease, see above.
For other conditions the risk of thyroid problems in infant is low
If hypoglycemia is unusually severe, or prolonged, or lacks an obvious cause...
Perform critical hypoglycaemia bloods (under Blood Tests) during an episode
A fetal ultrasound soft marker for aneuploidy
Found in 5 to 25 % of fetal scans (ethnicity dependent)
Represents mineralisation in papillary muscle
In the absence of aneuploidy there are no long term implications
Routine echocardiogram is not required
No increased risk of rhythm disturbance: no need for ECG
Complete a standard neonatal examination
No additional investigations or follow up required
Appropriate reassurance
A single green vomit in a newborn may be the only early warning sign of malrotation and volvulus
Perhaps 30% of infants with green vomit have a surgical pathology
Any delay in diagnosis of malrotation with volvulus can result in bowel loss
Although any colour of vomit can be serious we are most concerned about green vomitus
Compare with this colour swatch
Colours 5 to 8 are significant green vomits
Discuss urgently with neonatal paediatrician (including over night)
History / examination / AXR / gas / blood culture usually indicated
Urgent abdominal ultrasound or upper GI study often required
Consider sepsis
Consider other causes of bowel obstruction
Often no pathology is identified
Normal variants include:
In general follow up with GP
GP will review head growth and shape at 2 and 6 weeks
Neonatal Clinic Review is not required
If concerned about "red flags" as above, discuss with senior medical staff
A dimple or pit below the intergluteal crease
Sacral pits are rarely significant
Asymmetric intergluteal crease
Midline lipoma or vascular birthmark
Very hairy overlying skin
Base of pit not visible
Sacral ultrasound in 2 to 4 weeks
Follow up in Virtual Clinic
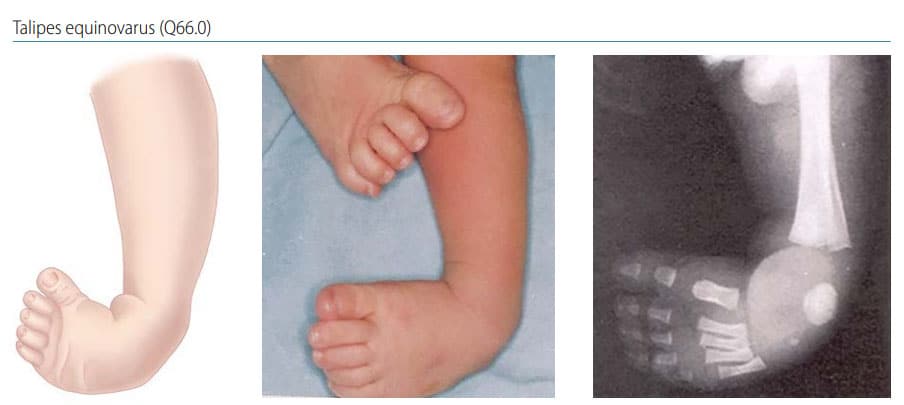
Physiotherapy referral pre-discharge
Early treatment with exercise / splinting improves outcomes
Casting and surgery may be required
Very mild positional talipes has a mobile foot easily manipulated into a normal neutral position
These cases may not need further referral
Discuss with neonatologist
Hypospadias
Microphallus
Excessive scrotal pigmentation
Hypoglycemia or hyponatremia
Testes may not reach scrotum till 3 to 4 months of age
Ultrasound to locate testes is not usually indicated
Document in the Blue Book
Recommend GP review at 4 months
Should be referred to Paeds Surgeon if not in scrotum by 4 months
Ostelin Infant Vit D Drops (2.4 mL) 400u = 1 drop
Pentavite (30mL) 400u=0.45 mL
Ostelin Vit D (50 mL) 1000u = 0.5 mL
All are purchased "over the counter" rather than prescription
Cost is similar for all the above (about $5 - $7 per month)
Easy to administer one drop = 400u
No bitter taste or bad smell
No unwanted extra vitamins
Doesn't stain clothes
80 doses per bottle
$10 - $15 (cheapest at "warehouse" pharmacies)
Term infant of appropriate birth weight: up to 10% weight loss is normal
Preterm infant or SGA infant: up to 7% weight loss is normal
Cesarean delivery increases the likelihood of > 10% weight loss
Flaherman et al Peds 2015 has detailed normative data on weight loss
Excessive weight loss is usually due to problems with lactation and breast feeding
Provide practical support for breast feeding
The SA PPG Breastfeeding is a very useful resource around breastfeeding, weight loss, and practical strategies.
Consider possible illness in infant
Discuss with consultant if weight loss 12% or more in term infant
Discuss with consultant if weight loss 10% or more in preterm or SGA infant
This app is designed to assist with your orientation to the Special Care Nursery and Women's Health wards.
Use this information alongside the relevant Practice Guidelines.